I. How to Use
When to Use
The YEARS Algorithm can be used in hemodynamically stable patients ≥18 years old with clinically suspected PE. It can also be adapted for use in the pregnant patient population.
Exclusion criteria include the following: patients who have had anticoagulation started 24 hours or more before assessment, a life expectancy less than 3 months, geographic inaccessibility for follow-up, or an allergy to an intravenous contrast agent.
Pearls / Pitfalls
Pearls
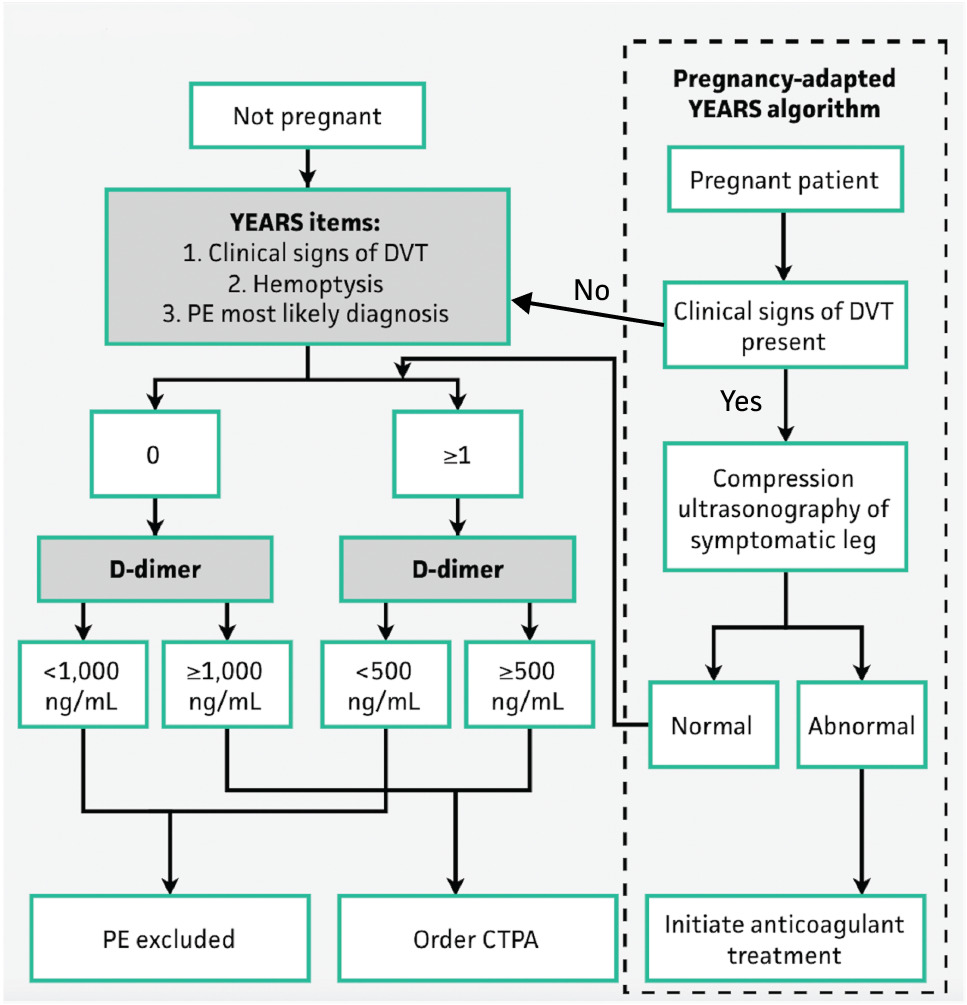
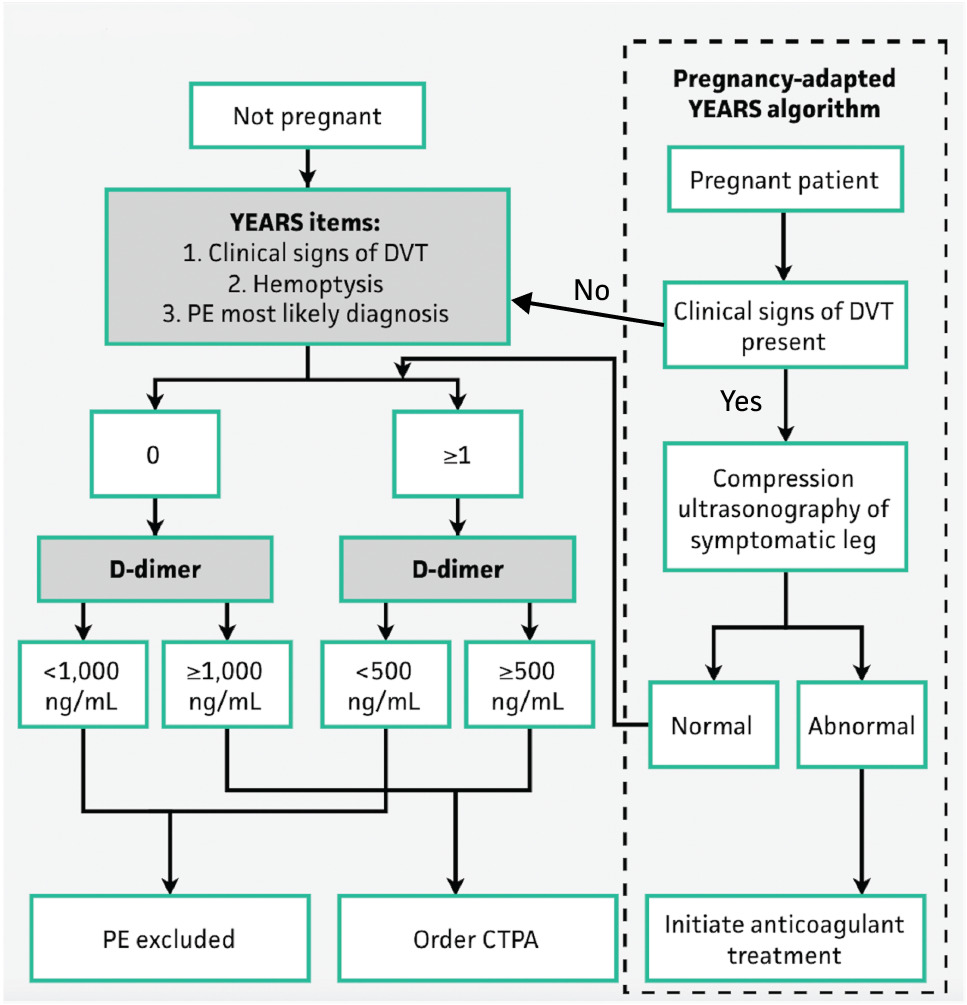
This tool uses three items from the original Wells’ Score for PE that were most predictive for PE: clinical signs of deep vein thrombosis (DVT), hemoptysis, and if PE is the most likely diagnosis.
It also applies a variable D-dimer threshold depending on the presence of one of the three items. If zero YEARS criteria are met, PE can be excluded if the D-dimer is <1000 ng/mL; in patients with ≥1 criterion, PE can be excluded if the D-dimer is <500 ng/mL. In all other patients, a CT pulmonary angiogram (CTPA) is recommended.
This tool can also be adjusted for use in pregnant patient populations. The pregnancy-adapted YEARS algorithm includes lower extremity ultrasonography as an initial step for patients with clinical signs or symptoms of DVT. If ultrasonography is negative and no YEARS criteria are present with a D-dimer <1000 ng/mL, PE can be safely excluded without CTPA.
Pitfalls
In order to use this tool, you must know your institution’s D-dimer assay units and input a correct conversion. The tool uses fibrinogen equivalent units with a unit of ng/mL.
The criterion ‘PE is the most likely diagnosis’ is inherently subjective and clinician-dependent. Because a positive response lowers the D-dimer exclusion threshold from 1000 ng/mL to 500 ng/mL, inter-clinician variability in its interpretation may meaningfully affect whether PE can be excluded without imaging.
Why Use
PE is a cannot-miss diagnosis. The YEARS algorithm safely reduces unnecessary imaging, radiation exposure, and contrast risk in a simplified manner while maintaining diagnostic safety when evaluating for PE. The index study for this algorithm (van der Hulle et al., 2017) demonstrated an absolute 14% decrease in the use of CTPA with use of this criteria, which has been replicated in validation studies, and an absolute reduction of 8.7% when using the age-adjusted D-dimer threshold for patients greater than 50 years old.
The YEARS algorithm has been evaluated and validated by multiple studies as well as adjusted to allow for use in the pregnant patient population.
II. Next Steps
Advice
The YEARS algorithm is a tool to use as an adjunct to clinical judgment and evaluation in the appropriate patient when considering PE as a diagnosis.
If the YEARS algorithm rules out PE:
- No further workup for PE is recommended.
If the YEARS algorithm is unable to exclude PE:
- Proceed with CTPA (or V/Q scan in patients where CTPA is contraindicated, such as those with iodinated contrast allergy, significant renal insufficiency, or in pregnant patients where minimizing radiation exposure to the fetus is preferred).
If there are clinical signs of DVT in the pregnant patient population, obtain compression ultrasonography of the appropriate leg first.
Management
If PE is confirmed by CTPA, initiate anticoagulation after evaluation of patient risk.
If PE is ruled out by the YEARS algorithm, continue your clinical evaluation and workup for other diagnoses as indicated.
Critical Actions
This tool should be used in hemodynamically stable patients.
Ensure that the appropriate D-dimer threshold is being used, depending on both the number of criteria positive and the units used by the institution.
The user needs to consider bleeding risk before initiation of any anticoagulation in patients found to have VTE.
This tool does not replace clinical judgment.
III. Evidence
Evidence Appraisal
The original YEARS study by van der Hulle et al was a prospective, multicenter cohort study amongst twelve hospitals in the Netherlands. The study created the YEARS algorithm from the Wells’ Score for PE and incorporated an adjusted D-dimer based on whether zero or one or more criteria are present. The inclusion and exclusion criteria for the tool come from the criteria used during the initial study: the inclusion of adults with age ≥18 years and the exclusion of patients with the following attributes: on anticoagulation greater than 24 hours prior to assessment, a life expectancy of less than three months, geographic inaccessibility that would prevent follow-up, an allergy to intravenous contrast agents, and pregnancy. All patients studied were hemodynamically stable. The study assessed the primary outcome of 3-month incidence of symptomatic venous thromboembolism (VTE) and a secondary outcome looking at the proportion of CTPA examinations performed per the algorithm.1
A total of 3465 patients were included in the study. 85% (2946) of patients had PE ruled out using the YEARS algorithm, and at 3-month follow-up, 0.61% (18 patients) were found to have symptomatic VTE, with 0.20% (6 patients) having fatal cases. Additionally, there was an absolute reduction of 14% of CTPA examinations using standard D-dimer thresholds and 8.7% reduction using age-adjusted D-dimer thresholds2 when comparing to a typical diagnostic algorithm using Wells’ Score for PE with a D-dimer result.1
This study demonstrated that the YEARS algorithm can be safely used to rule out PE in the intended population and reduce use of CTPA. The strengths of this study include the large patient population and ability to follow-up in 3 months for outcomes. Limitations for this study include the lack of control group, small number (43) of patients that deviated from the intended algorithm, and difficulty in determining if the presence of PE affected the death of patients during follow-up.1
This study has since been validated by Kabrhel et al, Freund et al, and Eddy et al identifying similar values for absolute reduction of CTPA and overall low failure rate of the algorithm.3-5 Eddy et al suggests caution in using this algorithm in patients with zero YEARS criteria and D-dimer results between the age-adjusted cutoff and 1000 ng/mL as patients in this category were found to have VTEs at 3-month follow-up in their study.5 Other studies of note include a systematic review by Te Haara et al that identified a sensitivity of 96% and specificity of 50% for the YEARS algorithm6 and a single center study by Duffy et al that also noted a reduction in the number of CTPA examinations completed without an increase in missed clinically significant PEs.7 Additionally, a study by van der Pol et al noted that using an age-adjusted D-dimer threshold did not add value to the YEARS algorithm. They found that when using this algorithm in patients of 50 years of age and older with at least one positive YEARS criteria, while there was a decrease in the number of required CTPA examinations, there was an increase in missed PE diagnoses.8
The YEARS algorithm has been safely adapted for pregnancy to include compression ultrasonography for pregnant patients suspected of PE with clinical signs or symptoms of DVT. A study by van der Pol et al demonstrated the ability to avoid CTPA in pregnant patients suspected of PE in 32-65% of patients (32% of third trimester patients, 46% of second trimester patients, and 65% of first trimester patients) through use of the YEARS algorithm with the pregnancy adaptation. Of note, the pregnancy-adapted YEARS algorithm was applied exclusively to patients with clinical suspicion for PE, rather than as a screening tool for patients with nonspecific chest symptoms.9 This adaptation has since been further evaluated and validated, demonstrating that it can safely exclude PE while reducing the need for radiation-based imaging in pregnant patients.10-12
Formula
Facts & Figures