I. How to Use
When to Use
ARISCAT is used in adult patients (>18 yrs) undergoing major elective and emergent non-cardiothoracic surgeries. Risk stratification is suboptimal in patients undergoing cardiac or thoracic surgery, specifically lung volume reduction, and should be avoided in these populations. Notably, the score maintains good predictive power in elderly patients >65 yrs old.
Pearls / Pitfalls
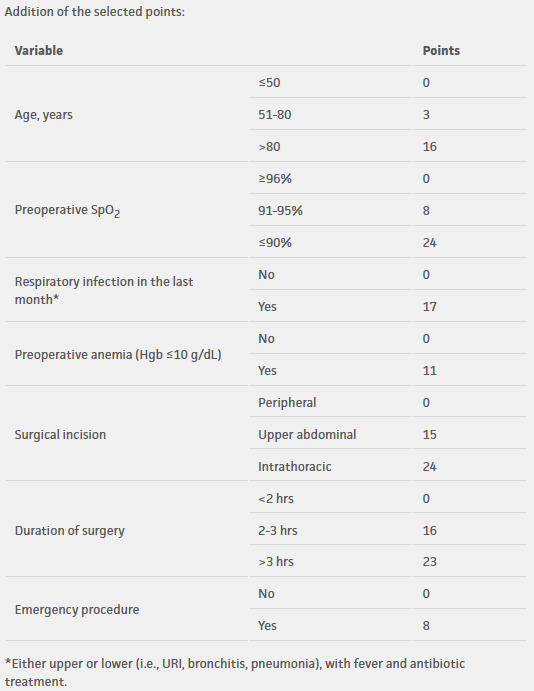
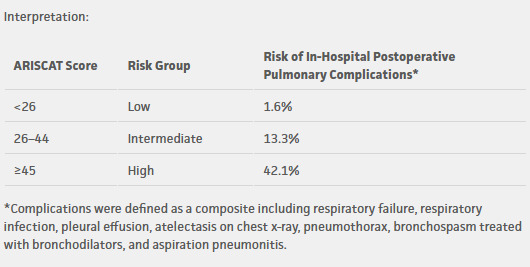
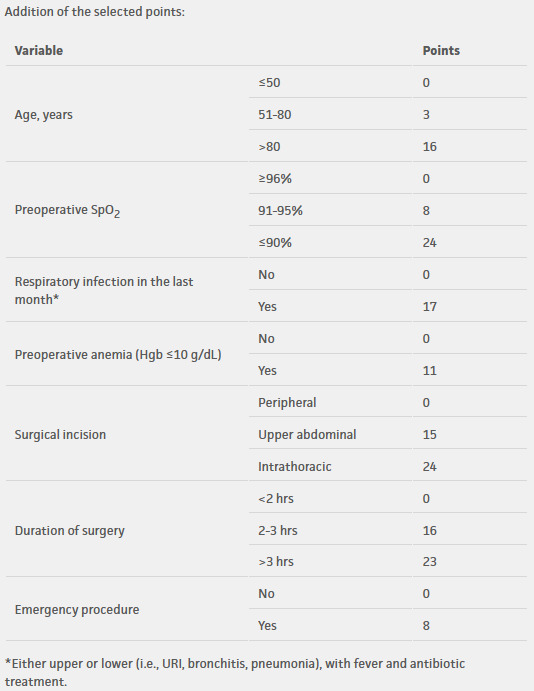
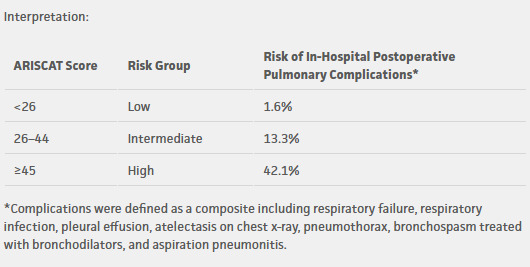
ARISCAT score should be calculated preoperatively by summing the risk factors (points in parentheses) to predict the risk of postoperative pulmonary complications: Age in years (<50 (0), 51-80 (3), >80 (16)), Preoperative SpO2 (>96% (0), 91-95% (8), <90% (24)), Upper/Lower respiratory infection within last month (No (0), Yes (17)), Preoperative anemia with Hgb <10g/dL (No (0), Yes (11)), Site of surgical incision (Peripheral (0), Upper abdominal (15), Intrathoracic (24)), Duration of surgery (<2 hrs (0), 2-3hrs (16), >3hrs (23)), and Emergent Nature (No (0), Yes (8)). The total score classifies patients into three different risk groups: Less than 26 is low-risk associated with 1-4% risk of postop pulmonary complications, 26-44 is intermediate-risk associated with 8-13% risk of postop pulmonary complications, and greater than 45 is high-risk associated with 38-42% risk of postop pulmonary complications. The score has been extensively validated for major emergency abdominal/urological surgery but demonstrates poor discriminatory ability in cardiac surgery and patients undergoing lung resections. Recently, it has been proposed that the ARISCAT overestimates risk due to the long duration of thoracic surgeries and elderly patient population (Hardavella). While ARISCAT facilitates risk-stratified perioperative planning, its impact on improving clinical outcomes remains uncertain.
Why Use
ARISCAT serves as a preoperative risk stratification tool that identifies patients at low, intermediate, and high risk of developing postoperative pulmonary complications allowing clinicians to consider risk mitigation strategies and heightened monitoring in the perioperative period. This score was the first externally validated, practical tool for identifying probabilities of these complications. Prior to this, clinicians would rely on assessment of individual risk factors (ASA status, symptom burden, presence of COPD, etc.) rather than a composite scoring system. This simple, bedside tool that uses multiple, objective data points filled a significant gap in the overall preoperative assessment.
II. Next Steps
Advice
The score performs best in non-cardiothoracic surgeries and is clinically limited in thoracic surgical populations; however, combining it with the presence of preoperative albumin levels <35g/L and ASA status may help identify high-risk patients. Formal NRI analyses and recalibration metrics have not been reported but may serve as an avenue of future research (Ulger). ARISCAT should be interpreted within the broader clinical context, including functional status, frailty, and psychosocial factors, especially prior to instituting mitigation strategies based on risk subtype. The score did show geographic variation in performance and is best calibrated for Western European populations. In the PERISCOPE validation study, there was a noted fall in calibration slope from 0.81 in Western Europe to 0.58 in Eastern Europe (Mazo). Limited U.S. specific validation studies should warrant caution when applying to North American populations.
Management
Though the evidence for ARISCAT-guided treatment comes predominantly from observational studies/expert guidelines and not RCTs, the recommended interventions have been validated in larger surgical populations allowing their reasonable application as risk-intensified perioperative measures rather than proven ARISCAT-specific therapy. The American College of Physicians outlines many of these recommendations in their 2006 clinical guidelines (Qaseem), but this document is best viewed as a foundational, non-ARISCAT specific reference that predates modern ERAS pathways. Many of the measures discussed are general pulmonary best practices independent of ARISCAT risk subtype with the score mainly helping determine how aggressively to prioritize optimization, monitoring, and post-operative respiratory support. For low-risk patients (<26), strategies may include standard perioperative workflows utilizing early mobilization, adequate analgesia to facilitate deep breathing and minimize atelectasis, incentive spirometry, and basic chest physiotherapy. Intermediate-risk patients (26-44) may receive all low-risk interventions plus preoperative optimization via smoking cessation, treatment of pulmonary comorbidities, and correction of anemia. Intraoperatively, recruitment maneuvers, careful use of paralytics with full reversal, and conservative fluid administration to avoid pulmonary edema have all been found to be helpful. In the post-operative period, aggressive pulmonary hygiene with incentive spirometry/chest physiotherapy, regional techniques to minimize opioids, and admission to step-down unit if a patient has marginal reserve can be considered. High-risk patients (>45) may receive all low/intermediate risk interventions plus consideration of inspiratory muscle training programs and optimization of comorbidities. Intraoperatively, high driving pressures should be avoided and time spent under general anesthesia minimized. Early institution of respiratory support (CPAP or BiPAP) in the post-operative period should be considered along with vigilant ICU monitoring in case reintubation is required.
Lung-protective ventilation with low tidal volumes (6-8mL/kg predicted body weight) combined with moderate/high PEEP has been shown to reduce incidence of post-operative pulmonary complications in broader surgical populations and should generally be viewed as standard of care. In certain patients, individualized PEEP strategies may offer additional benefit compared to a fixed PEEP level. The iPROVE-OLV trial found that PEEP titration to optimal lung compliance reduced postoperative pulmonary complications compared to standard protective ventilation in patients undergoing thoracic surgery (Ferrando). Inspiratory muscle training (IMT) is also a high yield intervention if instituted 2-8 weeks before surgery, particularly in patients with a higher baseline risk. The program usually consists of breathing exercises against resistance using a threshold inspiratory muscle trainer. Daily sessions are usually 15-30min and are done during the several weeks prior to surgery. A meta-analysis found that implementation of an IMT program reduces complications by 50% and shortens hospital length of stay by one day (Katsura). Specifically, high-risk patients derived the greatest benefit. Intermediate/low-risk patients also may benefit from IMT but the evidence is less substantial in these risk strata. Nevertheless, it is a low-cost and low-risk intervention that can be part of a larger preoperative optimization plan.
Critical Actions
The ARISCAT score only addresses risk of pulmonary complications and does not serve as a comprehensive perioperative assessment tool. Care should be taken to evaluate bleeding, thrombotic, cardiovascular, and procedure-specific risks simultaneously as these may take precedence over pulmonary optimization. Two specific situations that may alter pulmonary risk include:
-
Active pulmonary infection: Consider postponing surgery
- Active respiratory infection with fever only adds 17 points to the ARISCAT but may underestimate overall pulmonary risk in this context
-
Hypoalbuminemia: Consider nutritional optimization
- An important predictor of post-operative pulmonary complications and should trigger increased vigilance in the perioperative period
III. Evidence
Evidence Appraisal
Predictive Accuracy
The ARISCAT score was originally published in 2010 and sought to develop a risk assessment of postoperative pulmonary complications after surgery. The multicenter, prospective cohort study assessed over 2,400 patients in Spain given general, neuraxial, or regional anesthesia for scheduled or emergency surgery. The score provided three objective, verifiable variables (age, presence of anemia, and preoperative oxygenation level) along with surgical risk factors that could theoretically be readily predicted (incision site and surgery duration). For moderate-risk patients (score >26), the study found a sensitivity of 87.3% (95% CI 77.7-94%) and specificity of 79.1% (95% CI 77-81.1%). For high-risk patients (score >45), sensitivity was 61.9% (95% CI 49.7-73.2%) and specificity was higher at 96.5% (95% CI 95.5-97.4%). Additionally, study designers noted a c-statistic of 0.89 with their development subsample and 0.84 with their validation subsample (Canet).
The first validation study published in 2014 (PERISCOPE) was a similar multicenter, prospective cohort study of 5,099 patients across 63 European hospitals. The study attempted to measure how the score predicted postoperative pulmonary complications in a larger cohort. Overall, it found the scoring system had good discrimination (c-statistic of 0.80); however, a calibration drift was noted outside the derivation setting. Predicted versus observed postoperative pulmonary complications were 0.87% vs. 3.39% in low-risk patients and 7.82% vs. 12.98% in intermediate risk patients. It went further in determining that the positive likelihood ratio for pulmonary complications in the high-risk stratum (score >45) was 7.12 (5.93 to 8.56) compared to those with a lower score. Notably, the study found the score performed poorly in the Eastern European subset and advised clinicians to use the scale cautiously in differing geographical contexts (Mazo).
Subsequent validation studies in recent years have continued to support use of the ARISCAT scoring system. A retrospective cohort study of a single center in Colombia that looked at patients over 70 years old found sensitivity and specificity for the high-risk category was 77.1% and 67.9%, respectively with an AUC of 0.7867 (CI 0.737-0.834). The presence of a high-risk ARISCAT classification was significantly associated with the presence of postop pulmonary complications (OR 9.19, p <0.001) (Contreras-Arrieta). Similarly, a prospective Danish study following patients undergoing emergency abdominal surgery found that the score underestimated complication rates in this high-risk population (predicted 24.9% vs. observed 36.1%) but overall showed good discrimination with AUC 0.83 (95% CI 0.79-0.86) (Kokotovic).
Clinical Importance
The ARISCAT has shown promise in identifying high-risk patients for enhanced preoperative evaluation and optimization. A retrospective cohort study from Mexico found that patients deemed high-risk by ARISCAT score who also underwent preoperative spirometry had reduced mortality compared to those without spirometry. The authors attributed the improvement to better risk identification and preoperative optimization, though the observational design and selection bias limits causal inference (Mares-Gutierrez). The findings suggest that combining ARISCAT with spirometry and appropriate interventions may provide survival benefits, though further validation is needed.
Clinical Applicability
Larger, comprehensive studies yielded mixed results regarding ARISCAT use. A 2022 systematic review of patients undergoing major abdominal surgery noted that of six predictive models for postoperative pulmonary complications, the ARISCAT demonstrated the best discrimination (AUC 0.7, CI 0.683-0.717), but failed to meet the a priori threshold for good discrimination (AUC >0.7). Authors noted that although predictive performance may be insufficient for precise individual risk stratification, ARISCAT remains useful for identifying patients at low risk of postoperative complications (STARSurg). A 2025 meta-analysis looked at c-statistics across 14 previously validated models for predicting postoperative pulmonary complications noting high risk of bias in all using PROBAST criteria. This was primarily due to the retrospective nature of data collection, lack of cohort diversity, and absence of simultaneous analyses of model discrimination and calibration. Authors noted that the ARISCAT score demonstrated moderate discrimination with a pooled c-statistic of 0.76 (95% CI 0.67-0.86) and was the most extensively validated model with unchanged efficacy across different cohorts. Other models showed superior discrimination for specific complications: DAGDA for postoperative pneumonia and Yoon for respiratory failure. However, these models did not have many external validation studies. The Gupta respiratory failure model and NSQIP pneumonia model both demonstrate excellent discrimination (c-statistics >0.85) for specific, individual outcomes; however, lack of external validation studies and meta-analyses makes it challenging to compare them to the ARISCAT’s pooled c-statistic (0.76) that looks at composite outcomes across heterogenous surgical populations. Overall, the study authors found that there was sufficient evidence to support ARISCAT use in risk stratifying patients and guiding their care (Huang).
The ARISCAT score has been found to be suboptimal in thoracic surgery populations. A single-center, retrospective cohort study compared different pulmonary risk scoring systems: namely ARISCAT, LAS VEGAS, SPORC, and CARDOT. Authors found that none of the systems had adequate discriminatory power in predicting risk of postoperative pulmonary complications with a c-statistic of roughly 0.6 (Zorrilla-Vaca). Additional studies have found that combining ARISCAT with other clinical values might help predict overall risk. One study found that ASA III and albumin levels <35 g/L were significantly associated with post-operative pulmonary complications (p = 0.002 and p =0.007, respectively) and combining these two variables with high ARISCAT scores identified patients with higher rates of pulmonary complications (p=0.004) with subsequent delayed chest tube removal/discharge time (Ulger). Another retrospective cohort study of patients undergoing esophagectomies noted high ARISCAT scores were independently associated with postoperative pneumonia (OR 1.4, CI 1.22-1.6, p < 0.001) while a high prognostic nutritional index was protective (OR 0.79) (Zhang). For patients undergoing one-lung ventilation (OLV) for esophageal surgery, OLV duration for less than 150 minutes was associated with better outcomes and recommended to be considered in conjunction with ARISCAT risk stratification (Lai).
Usability
Overall, the ARISCAT scoring system has been useful in predicting likelihood of postoperative pulmonary complications. It remains an attractive bedside tool due to its simplicity in calculation from routinely available variables. Particularly, it has decent discriminatory power in identifying patients at high-risk. Nevertheless, it should guide risk stratification within the broader clinical context, rather than serve as the sole determinant of perioperative management. Additionally, the score should be used with care in certain patient populations, such as those undergoing thoracic surgery or one-lung ventilation, and additional clinical variables should be assessed including albumin levels, spirometry results, and ASA level.
Formula
No modifications to the original formula have been made since its initial publication and subsequent validation in the 2014 PERISCOPE study.
Facts & Figures
Literature
Original/Primary & Validation
Canet J, Gallart L, Gomar C, Paluzie G, Vallès J, Castillo J, Sabaté S, Mazo V, Briones Z, Sanchis J; ARISCAT Group. Prediction of postoperative pulmonary complications in a population-based surgical cohort. Anesthesiology. 2010 Dec;113(6):1338-50. doi: 10.1097/ALN.0b013e3181fc6e0a. PMID: 21045639.
Mazo V, Sabaté S, Canet J, Gallart L, de Abreu MG, Belda J, Langeron O, Hoeft A, Pelosi P. Prospective external validation of a predictive score for postoperative pulmonary complications. Anesthesiology. 2014 Aug;121(2):219-31. doi: 10.1097/ALN.0000000000000334. PMID: 24901240.
Contreras-Arrieta S, et al. Performance of the ARISCAT Score for Predicting Postoperative Pulmonary Complications in Major Abdominal Surgery in Elderly Patients. Colomb J Anesthesiol. 2025 Mar;53(2):e1140. doi:10.5554/22562087.e1140.
Kokotovic D, Degett TH, Ekeloef S, Burcharth J. The ARISCAT score is a promising model to predict postoperative pulmonary complications after major emergency abdominal surgery: an external validation in a Danish cohort. Eur J Trauma Emerg Surg. 2022 Oct;48(5):3863-3867. doi: 10.1007/s00068-021-01826-6. Epub 2022 Jan 20. PMID: 35050387.
Other References (including meta-analyses, CPGs, and impact analyses)
Hardavella G, Karampinis I, Salomidou M, et al. The Assess Respiratory Risk in Surgical Patients in Catalonia (ARISCAT) score overestimates postoperative complications’ risk in thoracic surgery. Eur Respir J. 2023;62(suppl 67):PA3879. doi:10.1183/13993003.congress-2023.PA3879
Huang Z, Han Y, Zhuang H, Jiang J, Zhou C, Yu H. Prediction models for postoperative pulmonary complications: a systematic review and meta-analysis. Br J Anaesth. 2025 Nov;135(5):1415-1427. doi: 10.1016/j.bja.2025.04.025. Epub 2025 Jun 4. PMID: 40473567; PMCID: PMC12597335.
Qaseem A, Snow V, Fitterman N, Hornbake ER, Lawrence VA, Smetana GW, Weiss K, Owens DK, Aronson M, Barry P, Casey DE Jr, Cross JT Jr, Fitterman N, Sherif KD, Weiss KB; Clinical Efficacy Assessment Subcommittee of the American College of Physicians. Risk assessment for and strategies to reduce perioperative pulmonary complications for patients undergoing noncardiothoracic surgery: a guideline from the American College of Physicians. Ann Intern Med. 2006 Apr 18;144(8):575-80. doi: 10.7326/0003-4819-144-8-200604180-00008. PMID: 16618955.
Zorrilla-Vaca A, Grant MC, Rehman M, Sarin P, Mendez-Pino L, Urman RD, Varelmann D. Performance Comparison of Pulmonary Risk Scoring Systems in Lung Resection. J Cardiothorac Vasc Anesth. 2023 Sep;37(9):1734-1743. doi: 10.1053/j.jvca.2023.05.035. Epub 2023 May 24. PMID: 37330329.
Mares-Gutiérrez Y, Martínez-González A, Salinas-Escudero G, García-Minjares M, Liu S, Flores YN. Combining Spirometry and the ARISCAT Respiratory Risk Assessment Can Improve Postoperative Outcomes and Reduce Mortality Risk in Mexico. Open Respir Arch. 2024 Apr 18;6(3):100325. doi: 10.1016/j.opresp.2024.100325. PMID: 38764716; PMCID: PMC11101723.
STARSurg Collaborative and TASMAN Collaborative. Evaluation of prognostic risk models for postoperative pulmonary complications in adult patients undergoing major abdominal surgery: a systematic review and international external validation cohort study. Lancet Digit Health. 2022 Jul;4(7):e520-e531. doi: 10.1016/S2589-7500(22)00069-3. PMID: 35750401.
Ülger G, Sazak H, Baldemir R, Zengin M, Kaybal O, İncekara F, Alagöz A. The effectiveness of ARISCAT Risk Index, other scoring systems, and parameters in predicting pulmonary complications after thoracic surgery. Medicine (Baltimore). 2022 Jul 29;101(30):e29723. doi: 10.1097/MD.0000000000029723. PMID: 35905198; PMCID: PMC9333546.
Lai G, Guo N, Jiang Y, Lai J, Li Y, Lai R. Duration of one-lung ventilation as a risk factor for postoperative pulmonary complications after McKeown esophagectomy. Tumori. 2020 Feb;106(1):47-54. doi: 10.1177/0300891619900805. Epub 2020 Jan 22. PMID: 31964281.
Ferrando C, Carramiñana A, Piñeiro P, Mirabella L, Spadaro S, Librero J, Ramasco F, Scaramuzzo G, Cervantes O, Garutti I, Parera A, Argilaga M, Herranz G, Unzueta C, Vives M, Regi K, Costa-Reverte M, Sonsoles Leal M, Nieves-Alonso J, García E, Rodríguez-Pérez A, Fariña R, Cabrera S, Guerra E, Gallego-Ligorit L, Herrero-Izquierdo A, Vallés-Torres J, Ramos S, López-Herrera D, De La Matta M, Gokhan S, Kucur E, Mugarra A, Soro M, García L, Sastre JA, Aguirre P, Salazar CJ, Ramos MC, Morocho DR, Trespalacios R, Ezequiel-Fernández F, Lamanna A, Pia Cantatore L, Laforgia D, Bellas S, López C, Navarro-Ripoll R, Martínez S, Vallverdú J, Jacas A, Yepes-Temiño MJ, Belda FJ, Tusman G, Suárez-Sipmann F, Villar J; iPROVE-OLV Research Network Group. Individualised, perioperative open-lung ventilation strategy during one-lung ventilation (iPROVE-OLV): a multicentre, randomised, controlled clinical trial. Lancet Respir Med. 2024 Mar;12(3):195-206. doi: 10.1016/S2213-2600(23)00346-6. Epub 2023 Dec 5. PMID: 38065200.
Katsura M, Kuriyama A, Takeshima T, Fukuhara S, Furukawa TA. Preoperative inspiratory muscle training for postoperative pulmonary complications in adults undergoing cardiac and major abdominal surgery. Cochrane Database Syst Rev. 2015 Oct 5;2015(10):CD010356. doi: 10.1002/14651858.CD010356.pub2. PMID: 26436600; PMCID: PMC9251477.
Zhang P, Chen Y, Xu Z, Qin T, Yang Y, Liu C, Zhao J, Xia H. Prognostic value of the ARISCAT score for postoperative pneumonia in patients with esophageal squamous cell carcinoma: a retrospective cohort study. Eur J Med Res. 2025 Sep 29;30(1):899. doi: 10.1186/s40001-025-03189-9. PMID: 41024281; PMCID: PMC12482326.