I. How to Use
When to Use
-
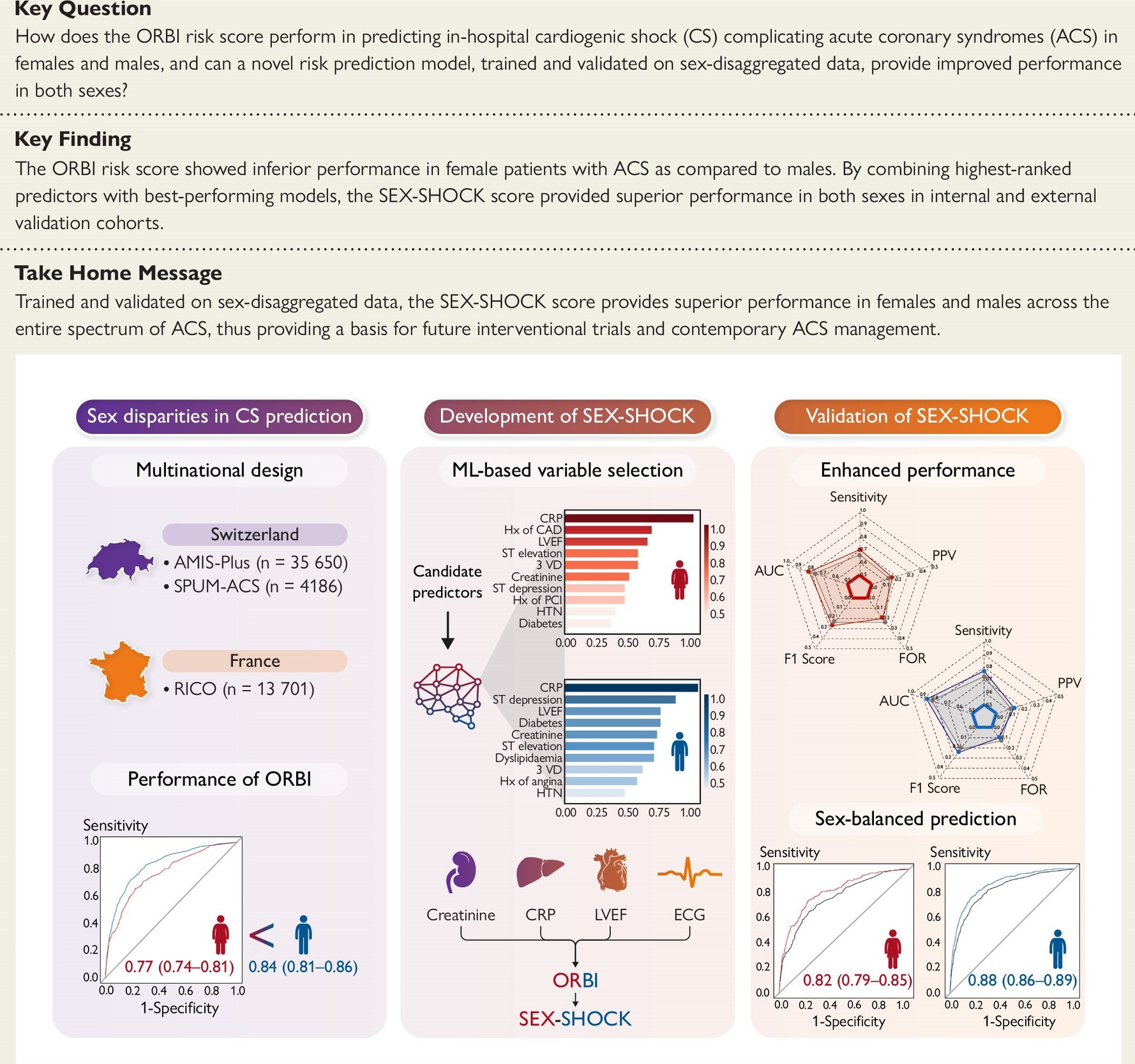
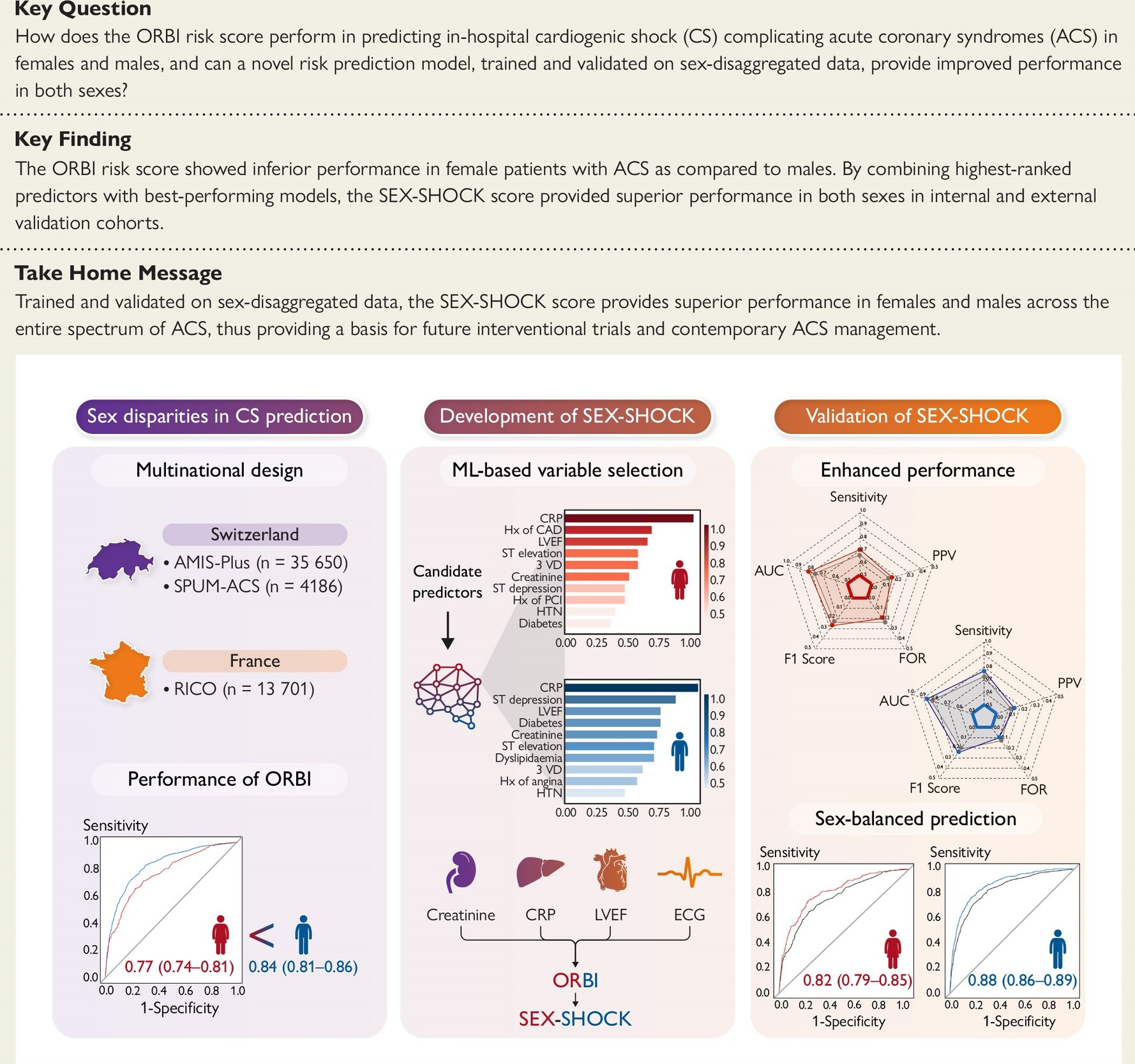
The first AI-assisted and sex-specific risk score to estimate the risk of in-hospital cardiogenic shock in patients presenting with acute coronary syndrome (ACS).
-
The SEX-SHOCK score is endorsed by the SCAI/EAPCI/ACVC and the HFSA.
-
Can be used in any patient with a working diagnosis of ACS, including both ST-segment elevation myocardial infarction (STEMI) and non-ST-segment elevation ACS (NSTE-ACS), who are planned for or have already undergone percutaneous coronary intervention (PCI).
-
Use caution when applying this score to patients who have not undergone PCI.
Pearls / Pitfalls
-
Estimates the risk for the development of in-hospital cardiogenic shock in both female and male patients with ACS who have not yet progressed to classic cardiogenic shock (i.e., SCAI-C or higher).
-
The original study derived and validated this tool in a European patient population, comprising a total of 53,537 patients with ACS, recruited between 2005 and 2022.
-
Does not consider factors such as ethnicity and other socioeconomic factors; caution should be used when generalizing the results to non-White populations.
-
Derived in ACS patients undergoing PCI. While external validation in all patients with ACS is pending, caution should be exercised if used in ACS patients not yet scheduled for PCI.
-
The (likely) time-dependent predictive performance over the hospitalization period was not assessed due to the lack of the exact time-point for in-hospital cardiogenic shock; calculated risk estimates should always be interpreted within the specific clinical context.
Why Use
-
Facilitates early identification of ACS patients at high risk for developing cardiogenic shock during their hospital stay, facilitating clinical decision-making regarding timely invasive management and closer monitoring.
-
May improve the early risk assessment of both female and male ACS patients.
-
Accounts for evolving ACS and cardiogenic shock management strategies, with the potential to personalize and improve contemporary ACS management.
-
Endorsed by the SCAI/EAPCI/ACVC and the HFSA.
II. Next Steps
Advice
-
To be used in conjunction with a detailed medical history and physical examination to help identify female and male ACS patients at high risk of cardiogenic shock, who may benefit from an early invasive approach and/or closer monitoring.
-
Always interpret SEX-SHOCK score results within the specific clinical context.
-
Incorporate clinical judgment and additional laboratory testing when determining a patient’s cardiogenic shock risk and potential benefit from emerging management strategies.
Management
- Note that randomized interventional trials, comparing management of ACS patients using best clinical practice versus best clinical practice and the SEX-SHOCK score have not been performed yet; thus, the benefit of using the SEX-SHOCK risk score to guide interventional management remains uncertain.
Critical Actions
-
External validation has been performed but is incomplete for all patient populations. Use caution when applying this score to patients who have not undergone PCI.
-
Note that randomized interventional trials, comparing management of ACS patients using best clinical practice versus best clinical practice and the SEX-SHOCK score have not been performed yet; thus, the benefit of using the SEX-SHOCK risk score to guide interventional management remains uncertain.
III. Evidence
Evidence Appraisal
-
Note that this score has high external validity given its development in a Swiss patient population (AMIS-Plus and SPUM-ACS) and external validation in France (RICO)
-
Shows superior predictive performance (across an array of performance metrics) as compared to other risk scores, including the ORBI risk score
Formula
Equations are as follows (sex-stratified β coefficients are listed in the table below):
SEX-SHOCK Score
Y = (Intercept) + β × log2(CRP mg/L + 1) + β × log2(Creatinine µmol/L) + β × ST-segment elevation + β × LVEF 35%-50% + β × LVEF >50% + β × Age >70 years + β × Presentation as cardiac arrest + β × Killip class III + β × Heart rate >90/min + β × SBP <125 and PP <45 mmHg + β × Glycemia >10 mmol/L + β × Culprit lesion of the left main + β × Post-PCI TIMI flow <3
Risk, % = [1 / (1 + e-Y)] × 100
SEX-SHOCKlight Score
Y = (Intercept) + β × log2(CRP mg/L + 1) + β × log2(Creatinine µmol/L) + β × ST-segment elevation + β × LVEF 35%-50% + β × LVEF >50% + β × Age >70 years + β × Presentation as cardiac arrest + β × Killip class III + β × Heart rate >90/min + β × SBP <125 and PP <45 mmHg + β × Glycaemia >10 mmol/L
Risk, % = [1 / (1 + e-Y)] × 100
Facts & Figures
Eur Heart J, Volume 45, Issue 43, 14 November 2024, Pages 4564–4578, https://doi.org/10.1093/eurheartj/ehae593
Literature
Sex-specific prediction of cardiogenic shock after acute coronary syndromes: the SEX-SHOCK score; Y Wang, M Zeller, V Auffret, G Georgiopoulos, L Räber, M Roffi, C Templin, O Muller, L Liberale, S Ministrini, K Stamatelopoulos, K Stellos, GG Camici, F Montecucco, H Rickli, M Maza, D Radovanovic, Y Cottin, F Chague, D Niederseer, TF Lüscher, S Kraler; Eur Heart J. 2024 Nov 14;45(43):4564-4578. doi: 10.1093/eurheartj/ehae593.
SCAI/EAPCI/ACVC Expert Consensus Statement on Cardiogenic Shock in Women; SJ Baron, JC Chou, T Shah, AR Vest, JD Abbott, M Alasnag, C Aurigemma, E Barbato, L Bellumkonda, AE Bortnick, A Chieffo, RJ van Geuns, CL Grines, S Halvorsen, C Hassager, NK Kapur, SS Naidu, VG Ng, J Saw, AJ Lansky; EuroIntervention. 2025 Aug 18;21(16):894-909; doi: 10.4244/EIJ-D-24-01126.
Acute coronary syndromes: mechanisms, challenges, and new opportunities; S Kraler, C Mueller, P Libby, DL Bhatt; Eur Heart J. 2025 Aug 1;46(29):2866-2889. doi: 10.1093/eurheartj/ehaf289.
Cardiogenic Shock; H Thiele, C Hassager; N Engl J Med. 2026 Jan 1;394(1):62-77. doi: 10.1056/NEJMra2312086.