I. How to Use
When to Use
This tool identifies patient factors negatively-associated with first-pass success in rapid sequence intubation.
Pearls / Pitfalls
The derivation study employed a retrospective review of air medical rapid sequence intubations, using expert consensus to categorize causes of failed first attempts into the six criteria. The major validation study was also retrospective and conducted in a similar aeromedical setting. Only one, smaller, validation study was prospective and in the emergency department.
Furthermore, they were not validated against any other system of airway assessment.1,2
Why to Use
Anticipating the difficulty of an intubation beforehand can help with risk-benefit analysis and for planning the optimal approach.
II. Next Steps
Management
With increasing HEAVEN criteria, the intubating provider may consider adjuncts such as video laryngoscopy or gum-elastic bougie. Or, the provider may want to consider alternative strategies such as delayed-sequence intubation or surgical cricothyrotomy.
III. Evidence
Evidence Appraisal
The HEAVEN criteria were derived to predict difficult airways in emergency rapid sequence intubation (RSI) and address limitations of prior tools like LEMON and Mallampati, which rely on cooperative patients and do not incorporate physiologic factors. Kuzmack et al. (2017) validated HEAVEN in a large air medical cohort, demonstrating that each criterion and the total number present were associated with decreased first-pass intubation success, particularly in high-acuity patients, supporting its utility for guiding airway strategy in emergency settings.
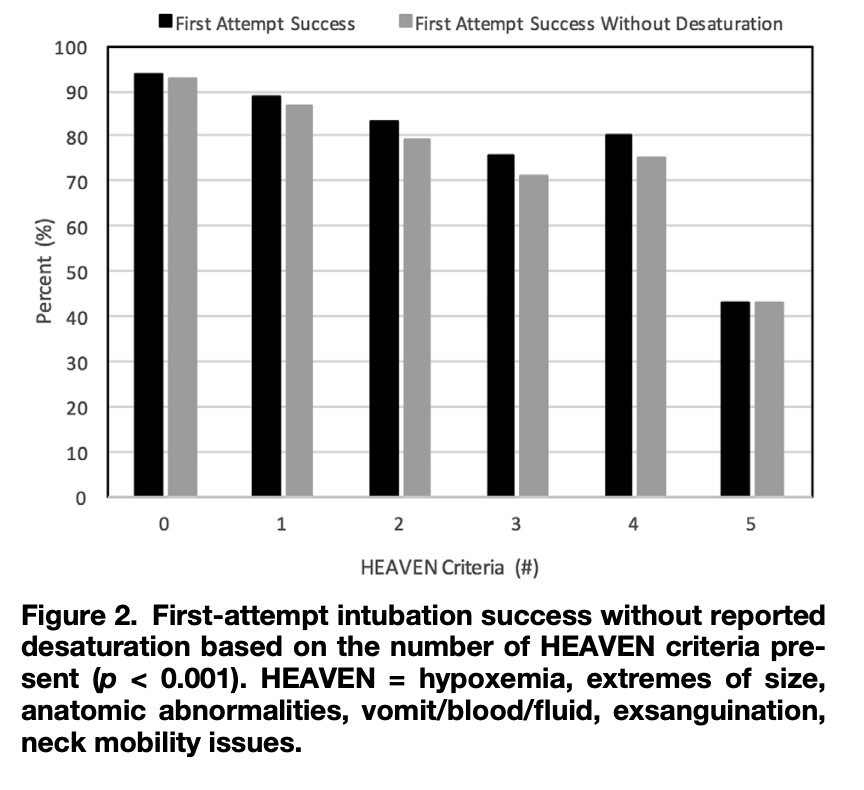
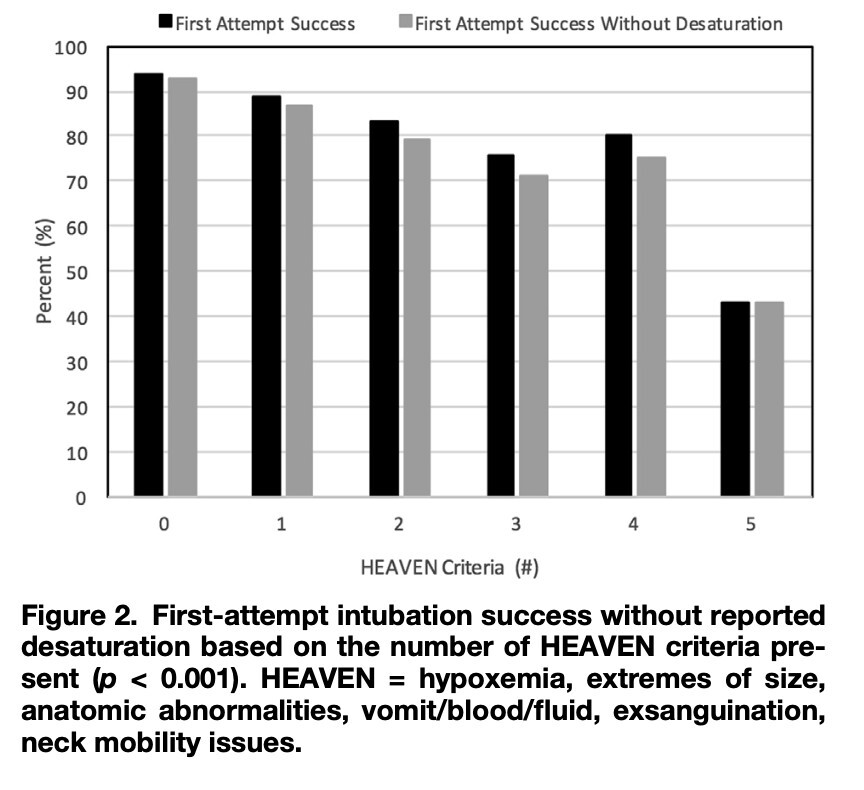
This study validated the HEAVEN criteria as a tool for predicting difficult airways during emergency rapid sequence intubation (RSI) in a large air medical cohort of 2,419 patients. Each HEAVEN criterion was independently associated with lower first-attempt success, and overall intubation success decreased as more criteria were present (from 94% with none to 43% with five or more). The criteria demonstrated high negative predictive value, supporting their usefulness for identifying difficult airways in emergency RSI settings. A follow-up study by Nausheen et al (2019) found similar conclusions after adding more than 2500 patients to the original cohort.3
Two letters to the editor critiqued the Nausheen et al. paper. Henschell et al. commented that the paper should have included optimal positioning of patients, especially with anatomical challenges like obesity. It also called into question why some physiologic criteria like exsanguination would correlate with difficult laryngoscopic views. Shao et al. questioned the predictive reliability of the HEAVEN criteria, noting that individual anatomic components sometimes had stronger associations with failed intubation than the total number of criteria combined. Both letters reinforced that HEAVEN is a predictive tool rather than a substitute for clinical judgment.4,5
Tan et al. validated the criteria in the emergency department with a prospective cross-sectional study involving 174 patients. Here also, the presence of any HEAVEN criterion was associated with first pass failure. With a much smaller sample size, only “anatomical challenge” was predictive by itself.6
Collectively, these data suggest that the HEAVEN criteria may be a useful tool for anticipating difficult airways during emergency RSI. While the evidence supports associations with difficult laryngoscopic view and decreased first-attempt success, the findings are primarily from specialized air medical settings with highly trained providers. As such, the generalizability to other clinical environments, patient populations, and provider experience levels remains uncertain. HEAVEN was calculated as an unweighted scoring tool. Given the importance of “anatomic challenge”, a weighted scoring system might have had greater predictive value, at the price of greater complexity. This could be a direction for further study. HEAVEN should be used to supplement, not replace, clinical judgment, and further prospective studies are warranted to evaluate its applicability across diverse emergency settings.
Formula
Each of the HEAVEN criteria (see Table 1) counts for 1 point, for a max of 6. The more criteria, the more challenging the airway is expected to be.
Facts & Figures