I. How to Use
When to Use
Used to determine low-density lipoprotein cholesterol (LDL-C) from a lipid profile collected from a patient when direct LDL-C is not obtained or measured (please see validation concerns prior to use).
Pearls / Pitfalls
The Modified Sampson–NIH LDL-C equation was developed to improve estimation of LDL-C, particularly at lower LDL-C levels, building on prior advances over the Friedewald formula. While analyses suggest improved performance within the derivation datasets, several limitations should be considered. The major limitation is that while developed and validated using large datasets from the Mayo Clinic and the FOURIER trial, the equation’s generalizability to diverse populations and clinical settings beyond these cohorts remains to be established through independent external validation. Its accuracy may be reduced when LDL-C levels exceed 300 mg/dL, making it less reliable in patients with very high LDL-C concentrations. Although it improves estimation near lower clinical LDL-C thresholds (55 and 70 mg/dL), its performance has not been validated for triglyceride levels above 1000 mg/dL or in conditions like dysbetalipoproteinemia, limiting its use in severe hypertriglyceridemia or rare lipid disorders. In patients with elevated triglycerides (≥400 mg/dL nonfasting), repeat fasting lipid measurements may help reduce variability associated with nonfasting states. As with all estimation formulas, it remains an indirect method and may not replace direct LDL-C measurement in complex cases or research contexts (e.g., very high triglyceride levels such as >1000 mg/dL and specific lipid conditions). The study may overestimate the accuracy of LDL-C equations because it first uses the gold-standard method β-quantification to define low LDL-C. rather than testing whether the formulas would have correctly identified those patients on their own. Additionally, the accuracy of different equations including Martin/Hopkins, Friedewald, and NIH-Sampson are debated (e.g., some studies suggest Martin/Hopkins may outperform NIH-Sampson (Samuel et al. 2023, Shi et al. 2022)
Why to Use
The Modified Sampson–NIH calculator could be considered for LDL-C estimation from a standard lipid profile. It improves treatment decisions by reducing misclassification at key clinical LDL-C thresholds (55 mg/dL and 70 mg/dL) compared to the original Sampson-NIH calculator and has been designed for triglyceride values up to 1000 mg/dL. Further validation, however, is necessary before widespread use.
II. Next Steps
Advice
Always input values in mg/dL to ensure correct calculation. The Modified Sampson–NIH equation suggests improved accuracy when LDL-C is low (<70 mg/dL) compared to the original formula but should be avoided if triglyceride levels exceed 1000 mg/dL, as it has not been validated in that range. Additionally, it should be used with caution as further external validation outside of the original cohort is necessary.
Management
LDL-C levels can be used to guide initiation and intensification of lipid-lowering therapy.
Treatment thresholds for LDL-C vary for primary and secondary prevention, along with patients with certain concomitant conditions (e.g., diabetes, coronary artery calcifications). Consider applying criteria from the 2018 ACC/AHA cholesterol guidelines or the 2022 ACC expert cholesterol consensus when deciding to initiate or intensify lipid lowering therapy.
Critical Actions
Not applicable.
III. Evidence
Evidence Appraisal
The Modified Sampson–NIH equation was developed using lipid panel data from the Mayo Clinic (n = 24,590) and the FOURIER trial (n = 9,605). Data were split evenly into training and validation cohorts. LDL-C was modeled against the reference standard β -quantification, using least-squares regression to optimize equation fit.
Designed to improve upon the original Sampson–NIH equation—particularly at low LDL-C levels—the modified version demonstrated superior performance. It achieved a concordance correlation coefficient of 0.992, outperforming the original Sampson, Martin–Hopkins, and Friedewald equations.
When assessed at key clinical LDL-C thresholds, the modified Sampson-NIH equation showed higher agreement by kappa analysis at both 55 mg/dL (κ = 0.98, P < 0.001) and 70 mg/dL (κ = 0.97, P < 0.001), compared to other equations (range: 0.92–0.96). It also demonstrated a lower false classification rate and improved correct patient classification by approximately 10–20%, supporting its utility in decision-making around lipid-lowering therapy.
A subsequent study by Meeusen and colleagues included 181 measurements from patients with triglycerides >=400 mg/dL or with triglycerides >=150 mg/dL and LDL-C<70 mg/dL. Modified Sampson-NIH had the highest correlation and least bias with beta quantification (median bias ~3-5 mg/dL) compared to Martin-Hopkins and direct LDL-C measurement. Overall, these data support the use of the modified Sampson-NIH equation, with well-validated performance for LDL-C determination. The study uses large, well-defined datasets with LDL-C calculations compared with gold-standard β -quantification.
Rating: The Modified Sampson–NIH LDL-C equation is a formula supported by lipid metabolism principles and derivation. It has been compared against gold-standard LDL-C measurements, demonstrating improved accuracy, particularly at low LDL-C levels and moderate triglyceride ranges (<1000 mg/dL). However, it assumes stable, fasting lipid levels and is less accurate in extreme hypertriglyceridemia. The formula, however, requires further validation as the original study used the same datasets for derivation and validation.
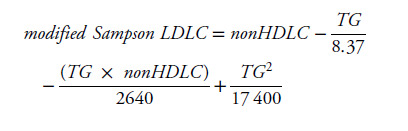
Formula
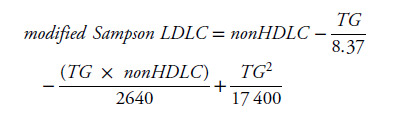
Facts & Figures
Not applicable
Literature
Original/Primary & Validation
Sampson M, Zubiran R, Wolska A, et al. A Modified Sampson-NIH Equation with Improved Accuracy for Estimating Low Levels of Low-Density Lipoprotein-Cholesterol. Clin Chem. Published online July 9, 2025:hvaf073. doi:10.1093/clinchem/hvaf073
Meeusen JW, Yi X, Nielsen JB et al. Modern Low-Density Lipoprotein Cholesterol Formulas Outperform Direct Methods in Patients with Hypertriglyceridemia and Low Levels of Low-Density Lipoprotein Cholesterol. Clin Chem. 2025 Sep 3:hvaf099. doi: 0.1093/clinchem/hvaf099.
https://pmc.ncbi.nlm.nih.gov/articles/PMC9604394/
Shi B, Wang HY, Yin D, Zhu C, Feng L, Wang H, Jia L, Fu R, Song C, Zhou Z, Lin Y, Song W, Dou KF. Comparison of Estimated LDL Cholesterol Equations with Direct Measurement in Patients with Angiographically Confirmed Coronary Artery Disease. J Cardiovasc Dev Dis. 2022 Oct 7;9(10):342. doi: 10.3390/jcdd9100342. PMID: 36286294; PMCID: PMC9604394.
https://pmc.ncbi.nlm.nih.gov/articles/PMC10289049/
Samuel C, Park J, Sajja A, Michos ED, Blumenthal RS, Jones SR, Martin SS. Accuracy of 23 Equations for Estimating LDL Cholesterol in a Clinical Laboratory Database of 5,051,467 Patients. Glob Heart. 2023 Jun 19;18(1):36. doi: 10.5334/gh.1214. PMID: 37361322; PMCID: PMC10289049.
Original Sampson-NIH Equation:
https://jamanetwork.com/journals/jamacardiology/fullarticle/2761953
Sampson M, Ling C, Sun Q, et al. A New Equation for Calculation of Low-Density Lipoprotein Cholesterol in Patients With Normolipidemia and/or Hypertriglyceridemia. JAMA Cardiol. 2020;5(5):540-548. doi:10.1001/jamacardio.2020.0013