I. How to Use
When to Use
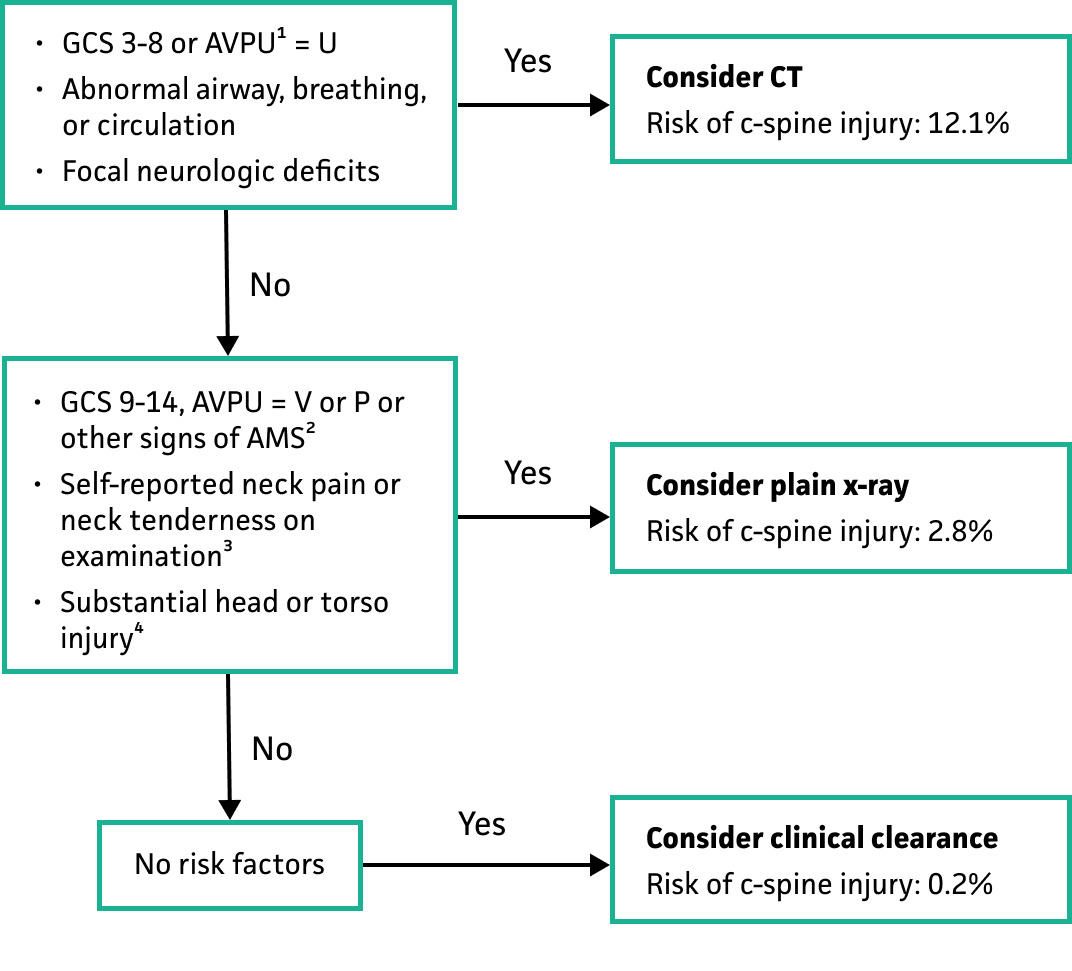
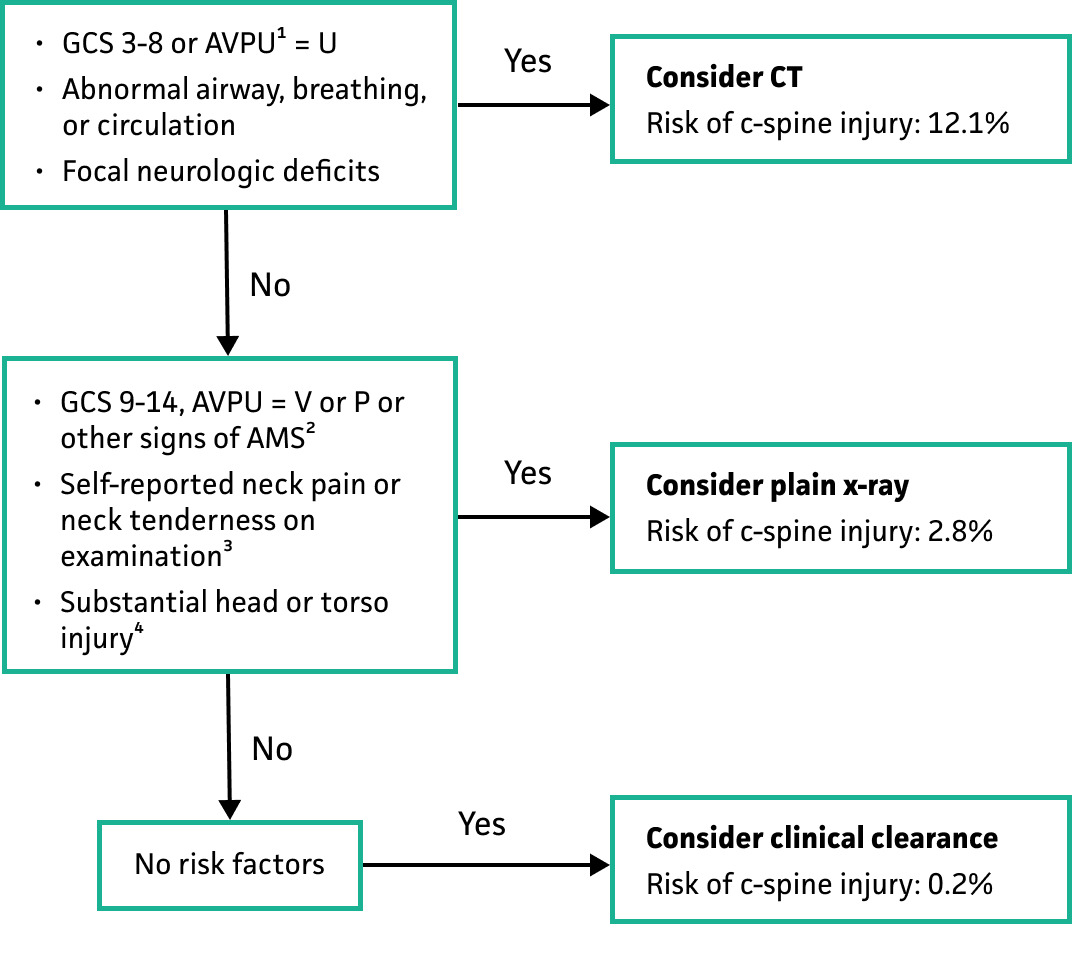
Use in pediatric patients (<18 years of age) presenting to the emergency department after experiencing blunt trauma. This tool can guide the determination for the necessity and choice of imaging.
“Substantial” head or torso injuries were defined as those injuries requiring inpatient admission or surgical intervention.
Pearls / Pitfalls
-
Demonstrated high sensitivity and negative predictive value for clinically significant injuries in the derivation study, making it a useful tool for ruling out cervical spine injuries.
-
The original study specifically excluded children with solely penetrating trauma.
-
Additional validation studies are currently in progress to further assess this tool’s effectiveness.
-
Children with conditions that predispose them to cervical spinal injuries, for example children with trisomy 21, are not covered by this rule.
-
While highly sensitive (94.3%), this rule should not supersede clinical concern for cervical spine injury.
Why Use
-
Helps minimize unnecessary and potentially harmful radiation exposure from imaging.
-
Unlike other cervical spine injury prediction rules, this tool was specifically developed for use in the pediatric population.
II. Next Steps
Advice
-
Always consider using the tool in conjunction with other clinical factors; it is meant to assist, not replace, clinical decision-making.
-
The original study notes that MRI may be required to clarify cases with a high pretest probability for cervical spine injury, although providing direct guidance was beyond the scope of that study.
Management
-
Cervical spine protection (cervical collar or other immobilization) should be maintained in children presenting with significant traumatic injuries until evaluated by a qualified physician
-
Do not avoid providing adequate analgesia for injured children in order to “preserve” a future neurologic examination
Critical Actions
- Children have a higher rate of “SCIWORA” (spinal cord injury without radiographic abnormality) than adults, meaning that an underlying spinal cord injury can be present even in the context of normal CT imaging findings. If a spinal cord injury is suspected (by a patient’s symptoms or physical exam findings), expert consultation with a pediatric trauma surgeon and / or pediatric neurosurgeon or spinal surgeon is recommended. Consider MRI to further evaluate for subtle spinal cord injuries that may be missed on CT.
III. Evidence
Evidence Appraisal
Leonard et al. evaluated children presenting with blunt trauma at 18 centers in the Pediatric Emergency Care Applied Research Network (PECARN) who underwent cervical imaging. Children presenting with exclusively penetrating trauma were excluded. A total of 11857 cases were included in the derivation cohort and 10573 children in the validation cohort. The primary outcome of interest was cervical spinal injury within 28 days of the initial injury requiring inpatient admission or surgical intervention. Children with suspected child abuse, children who were transferred from another institution, or in whom imaging results were known prior to data collection were excluded.
The presence of one risk factor in the decision rule was associated with a cervical spine injury in 12.7% (RR 8.9). The sensitivity of the rule was 94.3%, and the specificity was 60.4%. The negative predictive value was very high at 99.9%.
The limitations of this study are that it may exclude older children (as many pediatric trauma centers do not accept patients from the field older than about 14 years of age) and that it excludes certain traumatic mechanisms (specifically suspected child abuse). This rule has not been validated in such populations and should be applied with caution. The presence of conditions that may predispose children to cervical spinal injury, such as trisomy 21, does not factor into the PECARN rule. Predisposing conditions did not exclude children from inclusion in the derivation/validation cohorts, however the authors acknowledge that such data may be incomplete, and that the rule was designed to require only history & physical examination findings.
There is yet to be an external validation study, and it should be noted that both the derivation and validation cohorts were derived from the same data sets. This may limit generalizability, however the broad coverage of PECARN sites across North America and the large number of included children may mitigate potential bias.
The potential advantage is reduced ionizing radiation exposure, either by eliminating the need for any imaging (clinical “clearance” of the cervical spine only) or for a lower-radiation modality (plain X-rays instead of CT). This rule specifically includes pediatric patients only, increasing its validity in this population as compared to other cervical spine imaging rules such as NEXUS or the Canadian cervical spine rules.
Formula
Facts & Figures
As above.
Literature
Leonard JC, Harding M, Cook LJ, Leonard JR, Adelgais KM, Ahmad FA, Browne LR, Burger RK, Chaudhari PP, Corwin DJ, Glomb NW, Lee LK, Owusu-Ansah S, Riney LC, Rogers AJ, Rubalcava DM, Sapien RE, Szadkowski MA, Tzimenatos L, Ward CE, Yen K, Kuppermann N. PECARN prediction rule for cervical spine imaging of children presenting to the emergency department with blunt trauma: a multicentre prospective observational study. Lancet Child Adolesc Health. 2024 Jul;8(7):482-490. doi: 10.1016/S2352-4642(24)00104-4. Epub 2024 Jun 4. Erratum in: Lancet Child Adolesc Health. 2024 Dec;8(12):e17. doi: 10.1016/S2352-4642(24)00311-0. PMID: 38843852; PMCID: PMC11261431.