I. How to Use
When to Use
-
The first equation used to estimate kidney function for CKD staging.
-
The first equation used to adjust or discontinue medications based on kidney function.
Pearls / Pitfalls
-
Creatinine clearance calculated using the Cockcroft-Gault equation was used to approximate GFR clinically prior to the availability of current eGFR equations.
-
Creatinine clearance is the amount of blood completely cleared of creatinine in a minute and is usually an overestimate of GFR because of the tubular secretion of creatinine.
-
The original Cockcroft-Gault equation, derived in 1976, relied on non-standardized creatinine measurements and has not been updated with the use of internationally standardized creatinine measurements. It was derived to estimate creatinine clearance measured by 24 hour urine creatinine excretion in approximately 500 patients in a Canadian hospital of whom 96% were male. An adjustment factor was added for female patients.
-
Because it includes weight in the equation, the output of the Cockcroft-Gault equation is in ml/min (compared to MDRD or CKD-EPI, with output units of ml/min/1.73m2).
Why Use
-
While the Cockcroft-Gault equation was the first and is the most well-known estimating equation for kidney function, it has largely been replaced in clinical practice, with the MDRD and CKD-EPI equations performing better across a variety of populations.
-
These tools were developed in more diverse populations and are used to predict GFR developed in studies where GFR was actually measured. This overcomes the likelihood of creatinine clearance to overestimate kidney function.
-
While many drug dosing recommendations for patients with decreased kidney function were based on creatinine clearance calculations from the Cockcroft-Gault equation historically, it remains only one option for determining drug dosage and discontinuation. Newer medications and research utilize MDRD and CKD-EPI estimates of eGFR as they show better correlation with measured GFR than the CG equation.
II. Next Steps
Advice
-
The relationship between creatinine and kidney function is curvilinear with a greater decline in kidney function occurring as serum creatinine rises from 1 to 2 mg/dL as compared to from 4 to 5 mg/dL.
-
The curvilinear nature of this relationship results in the need to estimate kidney function using an equation that takes into account factors that reflect underlying muscle mass (and subsequently creatinine generation) that have been developed where kidney function has been actually measured.
-
Patients with decreased eGFR have kidney disease and are at higher risk of both acute kidney injury and progressive kidney disease. Management of modifiable risk factors, such as blood sugar and blood pressure control in diabetes mellitus and hypertension, is critical to slowing progression.
-
Medications should be dose-adjusted for the most recent available estimate of kidney function. In this setting, eGFR and creatinine clearance may be calculated and used similarly depending on the equation utilized when the medication was being developed, though they are physiologically different terms. Cutoffs for many medications are <60, <45 and <30 ml/min/1.73m2, as well as adjustments for advanced kidney disease and dialysis patients.
Management
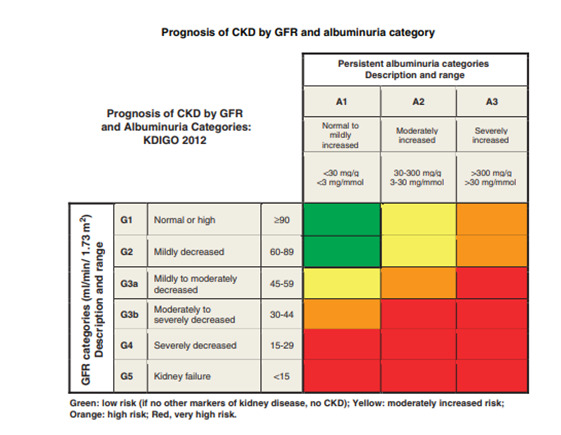
While creatinine clearance can be calculated, patients should be classified into CKD stage by both eGFR as estimated by either the MDRD or CKD-EPI formulae as well as the amount of urinary protein excretion. Patients with decreased eGFR, increased urinary albumin excretion or both, are at high risk of progressive CKD and should be referred to nephrology for further management.
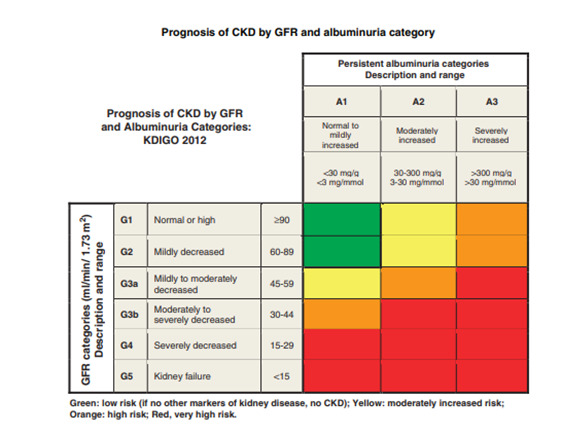
From KDIGO 2012 Clinical Practice Guideline.
III. Evidence
Formula
Cockcroft-Gault CrCl, mL/min = (140 – age) × (weight, kg) × (0.85 if female) / (72 × Cr)
Ideal body weight (IBW), Devine equation:
-
IBW, kg (male) = 50 + [ 2.3 × (height, inches – 60) ]
-
IBW, kg (female) = 45.5 + [ 2.3 × (height, inches – 60) ]
Adjusted body weight (ABW), kg = IBW, kg + 0.4 × (actual body weight, kg – IBW, kg)
Facts & Figures
The Cockcroft-Gault formula estimates creatinine clearance to clinically approximate glomerular filtration rate (GFR). Creatinine clearance, however, may over-estimate GFR by 10-20% and has largely been replaced clinically by equations to more directly estimate GFR.
Further, the Cockcroft-Gault equation uses body weight and is even less accurate in weight extremes (underweight and particularly overweight/obesity). As recommended by Brown et al and Winter et al, adjustments and estimates are made as follows:
Literature
Original/Primary
Cockcroft DW, Gault MH. Prediction of creatinine clearance from serum creatinine. Nephron. 1976;16(1):31-41. PubMed PMID: 1244564.
Other References
Winter MA, Guhr KN, Berg GM. Impact of various body weights and serum creatinine concentrations on the bias and accuracy of the Cockcroft-Gault equation. Pharmacotherapy. 2012 Jul;32(7):604-12. doi:10.1002/j.1875-9114.2012.01098.x. Epub 2012 May 10. PubMed PMID: 22576791.
Brown DL, Masselink AJ, Lalla CD. Functional range of creatinine clearance for renal drug dosing: a practical solution to the controversy of which weight to use in the Cockcroft-Gault equation. Ann Pharmacother. 2013 Jul-Aug;47(7-8):1039-44. doi: 10.1345/aph.1S176. Epub 2013 Jun 11. Review. PubMed PMID: 23757387.